Bovine TB Steering Group proposes change but offers little detail

Around two years ago, Daniel Zeichner, Labour’s then-new Defra Minister, described Defra’s large bovine TB department as being in a state of “civil war”.
Despite bovine TB control employing around 500 people and consuming much of Defra’s animal health budget, progress since 2010 had been sluggish when compared with the ‘all but’ done-in-a-decade control programme of the 1960s.
Changes at pace?
Zeichner promised “change at pace.” He commissioned a “Strategy Refresh” alongside a complementary review of scientific developments since the last review in 2018. The review was, as in 2018, led by Professor Charles Godfray with Professor Bernard Silverman, both of Oxford University, and others including Cambridge University vet James Wood. It reported in September 2025.
The 2025 Godfray panel report (see here) was notable for addressing some central issues of Defra departmental capability; a lack of leadership, and systemic weaknesses in the outdated immune-system-based cattle testing regime. However, it faltered badly on the crucial statistical analysis issues surrounding badger interventions.
Fresh leadership?
The panel called for fresh leadership. This reflects the Chief Vet and Deputy Chief Vet appearing overstretched, and the panel also requested significant additional resources and cooperation. But such requests were always unlikely to gain traction given Defra’s past struggle to deploy its existing resources effectively. Without both leadership and a workable plan, the report strongly implied, quite logically, that meaningful bTB control would remain out of reach for decades.
In fact, the original rationale for the costly cattle control and compensation system to protect human health, has long been recognised as unnecessary (see here and here). Yet no one appears willing to review that position or make the difficult but rational decision that could save future £ billions in public funds.
Propping up the RBCT while saying it doesn’t really matter any more?
On badger interventions, the Godfray panel accepted the Royal Society review (see here) saying that Torgeson et al (2024 & 2025) applied the more appropriate analyses of the Randomised Badger Culling Trial (RBCT) – the core policy science since culling began in 2013. They suggested that statistical methods in the original Donnelly et al 2006 analysis were not those epidemiologists would naturally use.
The collapse of the RBCT also undermined dozens of subsequent government-funded papers that relied on it, including calculations made in 2013, used in the 2018 review and several papers published since. Yet the Godfray report still reached the unconvincing conclusion that badgers were somehow significantly involved, perhaps because a lot of Godfray’s past work has assumed that the RBCT analyses were correct. He is now saying it doesn’t matter when it quite clearly does.
Problematic statistics?
The deeper problem lay with Professor Silverman’s binomial model in the Godfray review, which failed to recognise that the RBCT data involved double or triple counting individual herds that broke down consecutively during the study period (repeat breakdowns) (see here). It is therefore unsurprising that Silverman, Godfray and Defra declined to comment once concerns around statistical methods were raised privately. The basis of the Godfray panel’s attempt to revive the RBCT unravelled just as Defra was completing its ‘closed’ strategy consultations with selected contractors and industry interests in late 2025. Which is presumably why they froze independent scientists out of the co-design.
The refreshed strategy, originally expected in the New Year, was delayed first to spring and then to late spring. The reasons are unclear, but perhaps the failure to find adequate scientific support for the old RBCT conclusions was a significant factor.
An author of the original RBCT science paper, now a representative of the Zoological Society of London, is also a contractor for an NFU/Defra badger vaccination scheme. They are also a member of the goverments BTB Steering Group, and Wildlife and Countryside Link’s representative for NGO views on its BTB committee. There must surely be a conflict of interest here?
In October 2025, two of the old RBCT science authors and a PhD student submitted a revised version of the 2024 Mills et al. papers (here and here), but not a reply to the criticisms of it outlined in the Torgerson et al. Comment paper published in Royal Society Open Science in summer 2025. A year on, no reply has yet been published. It seems possible that the BTB Steering Group review was waiting for such a response, but it has been left with little choice but to bypass the 2025 Godfray panel’s finding, and revert to the Godfray 2018 review science, which is why it looks so outdated.
A new report with strategic recommendations
The Bovine TB Partnership of England Steering Group (see here), whose management has been widely criticised, has recently (June 10th) produced and presented A Bovine TB Strategy for England on TBHub (see here), apparently with strong direction from Defra. This is not a typical government response to a policy review. Instead, it is a proxy exercise by Defra-selected stakeholders working behind closed doors, with no public record and without the inclusive co-design promised to external scientists and nature conservation sector.
TBHub is a collaborative joint initiative between the UK agricultural industry and government. It was developed and is administered by the Agriculture and Horticulture Development Board (AHDB), who describe themselves as “the independent, impartial public body that unlocks success in British agriculture.” Not entirely independent, they receive project-based grants from Defra. Their heavily contested website contains considerable misinformation about bovine TB and wildlife. Despite complaints and promises from Defra staff to examine the issue, it has not been corrected, and continues to perpetuate misinformation.
Dame Angela Eagle (Minister at the time of the strategy release) confirmed that in relation to the strategy recommendations, Defra will:
“translate this strategy into action without delay, through a series of rolling three to five year delivery plans that ensure progress is sustained, transparent, and felt on the ground.”
However, there is still no clarity on how the effectiveness of badger vaccination will be measured, particularly important, given Defra’s inability to show in any shape or form, that it was badger culling that helped reduce cattle herd bTB breakdowns.
Godfray review ‘lite’
As a response to, or reflection of, the 2025 Godfray panel review, the new strategy report avoids the most difficult issues. It tries to reassure readers that the plan is clear by repeatedly saying so, while offering little detail on how or when delivery will happen.
Instead, it reads like a pep talk: “don’t look back”, “work together”, and wait for “promises down the line”. The result feels like another instance of the Government kicking the can down the road, because new leadership and resources are still needed. The problem is that Defra appears unable to make a sufficiently strong case to secure Treasury funding – and everyone knows it.
As a result, the document’s central sleight of hand fails immediately. Its graph showing bTB disappearing by 2038 is fanciful, if not insulting to those involved, given the lack of detail on how the disease is expected to fall sharply between 2027 and 2029 – before the proposed use of a cattle vaccine and DIVA test! Who came up with this when APHA said recently there was no prediction of when bTB would come under control?
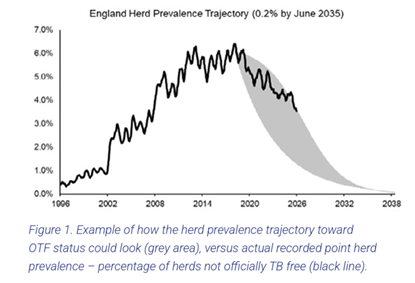
An alternative scenario that seems more probable;
Figure 2. Alternative example of how the herd prevalence trajectory toward OTF status could look (red area) given failure to vaccinate cattle due to an inadequate DIVA test and industry resistance to use of vaccine, but with widespread use of additional cattle tests such as Enferplex, Actiphage and Idexx.
What is Defra doing by putting out this new Partnership report?
Defra appears to be withholding what it actually intends to do, beyond buying time. This may begin with a bid for additional government funding from 2027, although current economic policy gives little reason to expect success, and with new cuts underway.
Defra is unlikely to significantly re-deploy the 500 staff working on bTB because it lacks the leadership to do so. Too many entrenched staff appear to be convinced that they already know the answers and may be difficult to retrain without fresh leadership. Effective trainers are also lacking and would themselves need specialist preparation. Real change must therefore start with new leadership at the top, capable of challenging old dogma, outdated thinking and mistaken assumptions.
Cattle vaccination – a major tool – is coming, or is it?
Central to the fantasy is the idea that a DIVA (Differentiate Infected from Vaccinated Animals) test will resolve the traditional industry block on use of vaccine. This was what an FoI to the Welsh Government came up with last December:
Question: “What is the target rate of specificity and sensitivity (reliability) of the test to differentiate between cattle vaccinated vs those infected with bTB before the Government is prepared to deploy it nationally?”
Response: “The primary screening test for TB in cattle in the UK and recognised by the World Organisation for Animal Health is the single intradermal comparative cervical tuberculin test (SICCT), or skin test. The Welsh Government understand the current studies aim to develop a test with a sensitivity and specificity which will be at least as good as, or better than the skin test.”
(Source: Welsh Assembly 2025 FoI response 8 December 2025 ATISN 26378 – Bovine TB See also claims of breakthrough: https://www.gov.wales/bovine-tb-vaccine-field-trials-major-breakthrough-long-term-plan-eradicate-disease-lesley-griffiths)
But the skin test has a sensitivity of only 50-80% at standard interpretation. Surely that will just not be good enough. Why are government still ignoring the infinitely more accurate phage blood tests that are available?
Given the long delay in developing a DIVA test (see here) and earlier claims of a breakthrough in 2020, the new report appears to overlook the practical reality. There is little reason to assume bTB incidence will change materially over the next three years, especially when existing incidence measures are themselves likely to be be unreliable, as bulk milk tank surveys suggest (see here).
The report should have acknowledged that cattle vaccination could require a temporary suspension of international live-cattle trade. The economic impact would likely be modest, particularly compared with the long-term benefits of effective disease control, but it would still need to be openly recognised and managed, given that the proposed DIVA test is unlikely to deliver the accuracy required for its stated purpose.
Action beyond cattle
One of the report’s most significant features is the absence of the proposals outlined by governments Deputy Chief Vet in Josh Loeb’s May 2026 Veterinary Record feature (see here and BadgerCrowd’s response here), i.e. targeted culling. After years of APHA misinformation, the report finally appears to accept that badgers are not a bTB maintenance host. However, this has been replaced by conclusions based on the now-questioned RBCT analyses.
This is particularly surprising because one of the original RBCT scientists, who is now on the bTB Steering Group, has co-authored several key papers that recent corrective science has substantially undermined. Yet the report does not acknowledge this. That ‘conflict of interest’ should have been declared. It is unacceptable for the report to cite many of the roughly 15 papers that no longer provide a reliable basis for future bTB control, because they recycle errors from the RBCT analyses (see list at end).
Page 20 also contains concerning and poorly explained statements about the Protection of Badgers Act 1992 and the Bern Convention. The example relating to badger vaccination is inappropriate, as there is no scientific evidence that it contributes to bTB control in cattle. The proposed framework for lethal control on page 22 is therefore unevidenced and risks becoming a major distraction from effective future bovine TB control.
On page 31, the report makes a statement that appears to ignore current scientific understanding of the RBCT and the derivative papers that repeat its problematic analytical methods:
This appears to contradict the Godfray review’s conclusions on these issues. Veterinarian James Wood served on both the Godfray review update panel and the BTB Steering Group, which makes the inconsistency more striking. The report does not acknowledge the review’s conclusions that the RBCT methods were ‘unnatural’, or that research that has been based on the results of the RBCT may no longer be relevant. Nor does it explain how this position can be reconciled with the many RBCT-derived papers that are similarly compromised, but cited in the review update.
James Wood’s long-standing support for government-funded badger culling makes this less surprising, but still disappointing. Many of the cited papers may eventually require correction, expressions of concern, or even retraction. For now, the Steering Group document seems to revert to the 2018 Godfray review position, when those papers were still treated as reliable. The conflict-of-interest concerns are therefore all the more problematic.
More troubling, this approach risks legitimising APHA staff who, since 2024, have argued for badger culling in Wales and Northern Ireland. By validating weak science, the report could help justify renewed badger killing in those administrations, while sidelining more accurate scientific understanding.
This points to a determined effort within Defra and among its chosen advisers to keep scientifically unsupported interventions available. The reasons are unclear, but may include a reluctance by key individuals to acknowledge earlier mistakes.
In 2022, BTB Steering Group chair John Cross told enquirers that the Partnership Group was not collectively equipped to evaluate scientific evidence. That raises obvious questions about why it was asked to lead this report and who actually drafted the text. As with the Godfray panel report, Defra appears likely to have played a major role in shaping the content and wording.
At the 9 June BTB Steering Group strategy launch at the Science Media Centre, several reports repeated the view expressed that people “should not look back”. In relation to the RBCT, that is untenable and rather suspicious: Defra’s policy framework is built around it, and that framework now appears to have collapsed, with Defra pretending it hasn’t. Between summer 2024 and summer 2025, the justification for culling, the business case, and the economic forecasts all fell away, and none has been replaced.
NGO misinformation
The Zoological Society of London (ZSL) web pages (see here) state: “We know that persistent bovine TB infections among wild badger populations are a contributing factor to the presence of the disease in cattle.” But this has not been established. The scientific evidence indicates that TB levels in cattle are independent of those in badgers, and that badger strains often do not match local cattle strains. Whilst some strains may be shared, transmission estimates remain highly speculative, and the overall contribution from wildlife likely too small for bTB control to have any effect on cattle breakdowns .
The ZSL strategy launch statement (see here) says: “While transmission of the disease from wildlife plays a small role in the persistence of the bTB, genome sequencing studies of the disease showing that around 17 times more transmissions occurred between cattle than comes from wildlife.” This makes use of one of the highly speculative genomic papers of recent years (Crispell et al 2019). It lacks the requisite data to be accurate and makes numerous uncheckable assumptions. Defra are trying to use it to replace the RBCT badger blame narrative. Effectively an attempt at a cover-up of past mistakes. Its just one bad decision after another, and all involved need to think again.

 In April, Farmers Weekly reported (
In April, Farmers Weekly reported (
 At the end of
At the end of  Worryingly however, Eagle apparently still referred to the need to maintain the ‘trust’ of the farmers via badger interventions. This seems to be an extension of Natural England’s decision in 2024 to continue badger culling, in order to provide the farmers with ‘clarity’. And going back further into the history books, it is the ‘carrot’ incentive for farmers to accept more regular bTB testing. A senior politician who spoke to vet John Bourne after the Randomised Badger Culling Trials (RBCT), was quoted as saying “Fine John, we accept your science, but we have to offer the farmers a carrot. And the only carrot we can possibly give them is culling badgers.” In other words, it looks very much like the badger remains a scapegoat for a cattle disease. Have we really not moved on after the unnecessary and cruel culling of a quarter of a million largely healthy badgers?
Worryingly however, Eagle apparently still referred to the need to maintain the ‘trust’ of the farmers via badger interventions. This seems to be an extension of Natural England’s decision in 2024 to continue badger culling, in order to provide the farmers with ‘clarity’. And going back further into the history books, it is the ‘carrot’ incentive for farmers to accept more regular bTB testing. A senior politician who spoke to vet John Bourne after the Randomised Badger Culling Trials (RBCT), was quoted as saying “Fine John, we accept your science, but we have to offer the farmers a carrot. And the only carrot we can possibly give them is culling badgers.” In other words, it looks very much like the badger remains a scapegoat for a cattle disease. Have we really not moved on after the unnecessary and cruel culling of a quarter of a million largely healthy badgers?

 Boyd suggested that there is continuing pressure to produce results to fit a political agenda, mistakes are commonplace, they continue to be made, and the way to prevent the same thing from happening in the future is far from clear. He wished he had known more about Bovine TB before taking on his role. You can read more about who said what
Boyd suggested that there is continuing pressure to produce results to fit a political agenda, mistakes are commonplace, they continue to be made, and the way to prevent the same thing from happening in the future is far from clear. He wished he had known more about Bovine TB before taking on his role. You can read more about who said what  Supplementary badger culling was authorized for a further year on June 1st. Natural England‘s scientific rationale for licensing did not take into account the
Supplementary badger culling was authorized for a further year on June 1st. Natural England‘s scientific rationale for licensing did not take into account the  On June 12th, a day later, the
On June 12th, a day later, the 
 On 13th October, there was a much awaited Westminster Hall debate (view
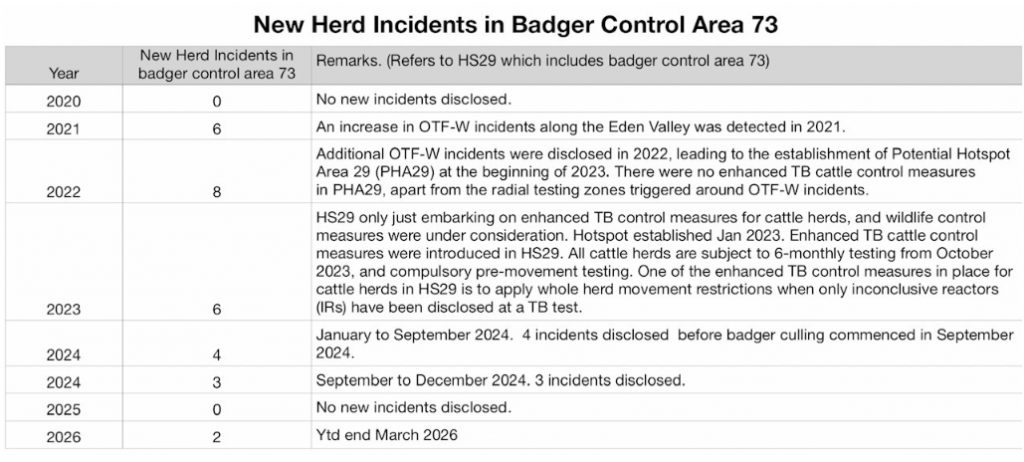
On 13th October, there was a much awaited Westminster Hall debate (view 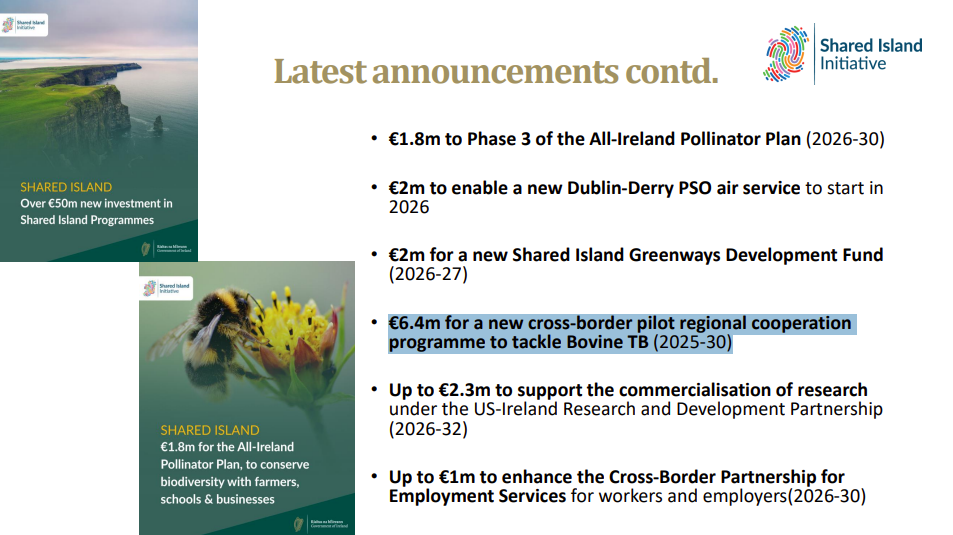 Meanwhile in Northern Ireland, a Parliamentary question by Miss Michelle McIlveen (from the DUP) tabled on November 18th made it clear that a €6.4m investment for a cross-border pilot regional cooperation programme on tackling bovine TB had been secured, with use of TVR as an experiment. This was leaked by the Ulster Farmers Union who wanted intensive badger culling and exposed DAERA’s attempt to instigate lethal interventions, despite previous undertakings not to do so without consultation.
Meanwhile in Northern Ireland, a Parliamentary question by Miss Michelle McIlveen (from the DUP) tabled on November 18th made it clear that a €6.4m investment for a cross-border pilot regional cooperation programme on tackling bovine TB had been secured, with use of TVR as an experiment. This was leaked by the Ulster Farmers Union who wanted intensive badger culling and exposed DAERA’s attempt to instigate lethal interventions, despite previous undertakings not to do so without consultation. A letter published 13th December in Vet Record (
A letter published 13th December in Vet Record ( It is thanks to all of you that we have collectively been able to protest, campaign, lobby, publish and report, and we can only hope that next year finally sees some truth and honesty from those who would seek to cover up the sins of the past. Particular thanks are due to all at Protect The Wild for their relentless public awareness work, especially the successful government petition and Westminster debate, backed by the general public. Also to Betty Badger (aka Mary Barton) and friends who maintained the Thursday vigil outside Defra offices, protesting the injustice (see article in the
It is thanks to all of you that we have collectively been able to protest, campaign, lobby, publish and report, and we can only hope that next year finally sees some truth and honesty from those who would seek to cover up the sins of the past. Particular thanks are due to all at Protect The Wild for their relentless public awareness work, especially the successful government petition and Westminster debate, backed by the general public. Also to Betty Badger (aka Mary Barton) and friends who maintained the Thursday vigil outside Defra offices, protesting the injustice (see article in the 
 The RBCT had three sets of trial areas; these were pro-active culling (badger density reduced by average 70%, reactive culling (100% culling around breakdown farms only), and no-cull control areas.
The RBCT had three sets of trial areas; these were pro-active culling (badger density reduced by average 70%, reactive culling (100% culling around breakdown farms only), and no-cull control areas. While badgers, like deer and other mammals both domestic and wild can be infected with bovine TB, the extent to which they may be responsible for a small proportion of cattle herd infections, especially in intensive livestock systems is unknown. If it occurs, there is no reliable data available that wildlife transmission to cattle can establish, maintain or perpetuate – this falsehood has been normalised by a few authors keen to bolster wrong claims. Indeed the
While badgers, like deer and other mammals both domestic and wild can be infected with bovine TB, the extent to which they may be responsible for a small proportion of cattle herd infections, especially in intensive livestock systems is unknown. If it occurs, there is no reliable data available that wildlife transmission to cattle can establish, maintain or perpetuate – this falsehood has been normalised by a few authors keen to bolster wrong claims. Indeed the